All
About FSR:
Questions and Answers
What does FSR mean and why?
FSR is the newest of AN treatments; it means Fractionated Stereotactic
Radiosurgery. It is a scientifically-based combination of two well-proven
techniques:
(1) stereotactic radiosurgery, a proven single-session procedure where the radiation field is
concentrated right on the tumor and is very weak in other parts of the brain;
(2) fractionated radiotherapy, which is what has bee used to treat brain cancer
for a long time, where many
treatments are used instead of one.
How does each one work separately?
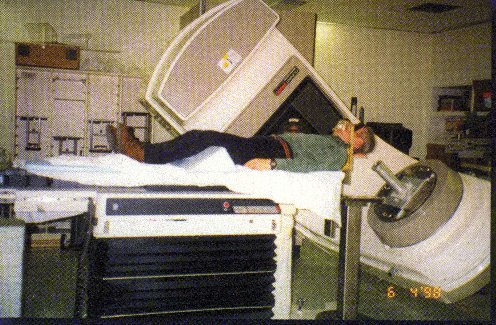
(1) This works either by having many rays converge on one point, as in Gamma Knife, or by
having one ray move in an arc, with the tumor at the center (here
is a photo of FSR treatment with such a machine). One has to make sure to carry out
the calculations and position the head just right, so the tumor is indeed in the center
and the healthy tissue is not; when some healthy tissue gets into the "hot zone"
the result is the negative statistics that radiosurgery is not immune from.
Gamma Knife has been
around since mid-1960's, with thousands of patients treated, so the long-term effects of
radiosurgery are no mystery - they are certainly no worse than well-performed surgery, for
many smaller tumors.
(2) In cancer, tumor cells migrate all over and irradiation of healthy tissue is
unavoidable. Fortunately, at lower doses, the tumor tissue responds more readily to
radiation that the healthy tissue, or rather does not recover as well from it as the
healthy tissue does. When treatment is fractionated, any single dose is too small to hurt
healthy tissue but between them all, the unhealthy tissue is deactivated just as with
radiosurgery. With many cancer patients around, doze calculations are an established
science.
Why combine the two?
It's pretty obvious - to reduce the chance of damage to healthy tissue to virtually nil.
Also, to enable the use of non-invasive treatments for any size and shape of ANs, even
where single-shot is counter-indicated due to the larger chance of getting healthy tissues
into the hot spot.
Why is FSR so recent then, if its benefits are obvious?
Implementing this combination relies on being able to reproduce the precision of
radiosurgery-type hot-spot positioning every time the patient comes back for treatment,
without screwing a frame into his head and recomputing everything each time. The following
advances in technology enabled this to be achieved:
(1) heavy use of computers and robotics
(2) custom-made masks or mouthpieces whose placement on the patient is simple and
non-invasive, yet gives the machine a chance to precisely locate the tumor for every
treatment.
How does the typical treatment look?
Here is the description of the treatment, from the doctors at John Hopkins;
other places are simular:
1-simulation with CT scan to acquire data regarding bone landmarks and to create the face mask to reproduce the position;
2-acquisition of highest quality MRI images for soft tissue definition (tumor and normal structures);
3-fusion of CT and MRI to obtain the most precise information and tridimensional definition about bone and soft tissue landmarks;
4-the data from the previous step in entered in the treatment planning software to allow the dosimetrist and the physicist to prepare a treatment plan;
5-the treatment plan is reviewed and corrected by the physicians, then signed;
6-the radiosurgeons with the set-up of the treatment, which is then completed by the technologist.
How many fractions, or doses are used?
There are 3 basic treatment modalities (protocols) for FSR:
The first protocol is in-hospital, since it requires a GK-type attached frame; the other two are outpatient, with a detachable frame. The protocols for individual FSR providers are listed in the Radiosurgeon Directory next to their contact information.
How is proper repositioning of the frame assured?
To assure proper positioning for every session, custom-made frames are used;
they come in two types:
Here are a few hints about the mask:
Here are patient testimonials about masks:
I was very surprised about how fast the mask hardened. One moment it was soft and a little pliable, the next, rock hard.
The technician who made and fit the mask said it was put together in 4 pieces. Mine had a seam which was quite bumpy on my nose and was extremely painful when the mask was connected and tightened; my nose was swollen and red. After the second session I asked the radiation technician if anything could be done and he smoothed the seam a little.
What happens to hearing after FSR?
Hearing and balance have been known to improve after FSR for some
patients. (Here is an informal survey that
confirms it.)
Mine was treated by radiation. Yes it's still in there. But I can stand to know the tumor is getting smaller and smaller each day and I have more hearing back than when I first had the radiation.
Hearing loss after FSR, if any, is gradual and usually partial -- some hearing usually remains. The choice of protocol makes a difference for avoiding hearing loss. Here is from Dr. Lederman:
"At the 2001 meeting I reported that days of treatment make a difference. Treatment on consecutive days results in a 50 percent stable or improved hearing rate compared to baseline, whereas alternate day treatment results in 80 percent stable or improved hearing rate".
Sudden hearning loss is also possible, but is should not be taken for granted! This is reversible with the use of steroids; you can read more about them here.
Does the tumor die right after FSR?
No, it first swells, before dying and shrinking. Noticeable swelling occurs
in at least half the patients, and does not indicate tumor growth.
In cases where the swelled tumor presses on the brain stem, symptoms will
be pronounced and steroids may be needed to keep the swelling down:
I had GK. I had balance issues and double vision so I was put on Decadron for a couple of weeks and then weaned off of it. The steroids increased my appetite, gave me more energy, but kept me from getting enough sleep. I had some weight gain. I was off the steroids for a while, but my symptoms returned. I was even starting to have trouble swallowing some foods. My doctor put me back on the steroids but at a lower dosage this time. I only take 2 mg twice a day. He explained that the radiation was causing the tumor to swell and press against the brain stem, therefore making the symptoms more pronounced... I have another MRI [coming up] and am hoping to be able to get off the steroids soon.
Sometimes, patients treated by radiatiosurgery are followed by ENTs or surgeons unfamiliar with this procedure, who mistakenly decide it was a failure and insist on surgery -- because they interpret the swelling as further growth. Therefore, it is very important to be aware of the swelling, and to maintain contact with the treating radiosurgeon on decisions such as whether further surgery is needed.
The swelling typically occurs 2-3 months after treatment. Here is a typical progression, for an FSR patient:
02/02: 2.2cm x 2.1cm x 2.0cm, initial diagnosis
07/02: 2.7cm x 2.1cm x 2.7cm, immediately pre-FSR
10/02: 2.9cm x 2.1cm x 2.9cm, 3 months post-treatment
12/02: 2.9cm x 2.1cm x 2.9cm, 5 months post-treatment
07/03: 2.1cm x 1.9cm x 2.1cm, one year post-treatment
It may take longer than a year for the swelling to subside. A Japanese study of GK patients showed that it can take up to 2 years (American Journal of Neuroradiology, Sep. 2000, pp. 1540-1546).
Are complications possible?
Three types of problems are possible after FSR:
More serious complications are possible, but extremely unlikely. For example, the machine might be out of whack (improper maintenance). Or, the MRI might not have been taken properly (incorrect shape determination). But one cannot discount FSR because of these possibilities just as one cannot discount the skills of an excellent surgeon just because he might have a bad fight with his wife on the morning of surgery. FSR causes no complications when done properly.
What size tumors can be treated with FSR?
Patients with larger tumors (usually
over 3 or 3.5 cm, depending on the radiosurgeon) are discouraged from FSR due to
increased risk of hydrocephalus as a result of
post-treatment swelling. However, there are exceptions:
I met an older lady yesterday at my AN support group that had a 4 x 2.5 x 2.5 cm. tumor treated with FSR as she didn't want to deal with surgery. Now 4 years later her tumor is 2.8 x 1.5 x 1.5 cm and she looks and feels GREAT.
[Editor's note: tumors are not shoes and do not come in exact sizes. This woman's original tumor size was most likely under 4 cm, between 3.5 and 4]
Is it possible to have repeat FSR?
Dr Lederman, who does not think there is any inherent danger in repeat
radiosurgery, does NOT treat the same AN twice anyway (in the few cases in which
the first treatment has failed to work). This is NOT because you can't,
but because he reasons that if a first treatment has failed, then a second one
is no more likely to succeed. Therefore, it is sensible to go to a top surgeon
at that point.
I have a 4mm AN; please comment on the following note I got from my GK provider: "We have not recommended fractionated radiation for tumors this small due to targeting concerns."
Having never heard of such concerns, we consulted with Dr. Jeffery A. Williams, Director of Stereotactic Radiosurgery in the Department of Neurosurgery at the Johns Hopkins Hospital. He wrote: "There are no targeting concerns for the FSR for the 4 mm AN."
What other FSR resources are available in the AN Patient Archive?
Questions to ask during your FSR consultation
Am I a candidate for FSR (Fractionated Stereotactic Radiosurgery)?
What is the procedure and steps in the treatment plan?
Do you have statistical data regarding treatment
results among your patients with tumors of similar size to mine as to:
A. Hearing acuity
post-treatment: six months; one year; two years; three years?
B. Headaches?
C. Balance Problems?
D. Dry Eye?
E. Facial Problems
After treatment when will I see any results in the shrinkage of the neuroma?
How likely am I to develop hydrocephalus? What would happen in this case?
What types of problems am I likely to experience as a result of tumor swelling after radiosurgery? When? For how long?
If I have headaches or a sudden loss of hearing do I contact you?
Can I have my MRI follow-up done at my home or hospital? What do I do then? Send them with an Audiogram to you for a report?
Is there an optimal time for treatment? Is there an optimal size for treatment?
What treatment would he choose if he had an AN your size? Why? When?
Last Edited: Wednesday, November 19, 2003
{kind=link}